
The Whole Genome Screening project - The London Genetics Centre Study (90S Study).
It is the first of its type to be based in a General Practice in the UK, as part of a Medical combined with an Echocardiogram and Ultrasound screening. It is a joint venture led by Professor Ros Eeles and Dr Michael Sandberg, together with consultants from The Royal Brompton Hospital. We have an international steering committee, composed of experts in different aspects of genetics, screening and ethics for the small initial pilot project which has now progressed into a larger Audit Study.
Screening healthy people with no significant medical family history and with Whole Genome Sequencing (WGS) is a new concept in preventative and personalised medicine.
Until now, only patients with a strong family or personal history of disease have seen. With technological advances and greater understanding of genes we are now for the first time able to open up genetics to a wider audience.
DNA double helix and sequencing output. Credit: Peter Artymiuk. CC BY
(Click to enlarge)
How can understanding your genome help improve your health planning?
Our genome is the blueprint that defines who we are.
We may have genetic vulnerabilities which combined with environmental health factors can put us at risk of diseases. Genetic screening is done to identify such gene alterations. This information can then assist GPs in personalising the patient’s health management, providing proactive and preventative healthcare for each individual tailored to genetic risk.
What is Whole Genome Sequencing (WGS) and why is it important?
Whole Genome Sequencing is the process of determining the complete DNA sequence of an individual’s genetic matter. Genes are small chunks of genetic information that we inherit from our parents. The human genome consists of approximately 20,000 genes, made up of 3 billion chemical building blocks, which are represented by combinations of the letters A G C and T on genetic test reports. The sequence of these letters reveals the individual’s unique code.
Other parts of the genome do not contain genes; they are noncoding and were formerly thought to be ‘junk’. Alternations in these regions may still have an impact on our health, by affecting a nearby or even more distant gene(s).
The whole genome – what is it?
Genetic dictionary basic concepts – see video link
www.genomicseducation.hee.nhs.uk/education
What percentage of people will benefit from genetic screening?
With our specifically chosen techniques, if we screen 100 people in a room we expect to find 5-6 people with significant actionable genetic variants.
SNP Profiling (Single nucleotide polymorphisms)
We will also identify another 5-6 people who will be at potentially 5-6 times greater risk of certain conditions by using a technique, called SNP profiling. Where the alterations are often outside the genes but still within the person’s genome. Single nucleotide polymorphisms (SNP) individually usually cause only a minor increased risk of a disease but if multiple SNPs are found, their cumulative risk of a particular disease may be up to 5-6 times the population risk.
In total we could identify up to 12% of people with key genetic life changing information
SNP profiling means that we will know which patients can be offered new trials of targeted screening programmes dependant on their SNP results.
The main causes of serious illness and premature death are Heart disease and Cancer. The incidence of both conditions is determined to a large extent by genetics and other risk factors. The London Genetics Centre has chosen a team of consultant geneticists in cancer medicine, cardiology, general and paediatric genetics. There are only about 250 consultant geneticists in the UK.
Genetics is an intricate science so you need a Genetics team which is at the cutting edge, wise, very experienced and gives great attention to detail. This is where The London Genetics Centre stands out.
What is the importance of doing Whole Genome Screening together with a medical.
The paradigm of medical diagnosis has always been to take a full history, including family history, to examine and then do basic investigations, prior to more specialised tests. This system remains fundamental to best medical care, despite the passage of time. Genetic screening, done in isolation, is just like having only one piece of a whole jigsaw puzzle.
What are actionable genes and why is it helpful to identify them?
A crucial part of healthy population screening is choosing of the right actionable gene list. ‘Actionable genes’ are genes in which inherited alterations are associated with a significant, but preventable, disease risk. Our team has carefully chosen over 650 actionable genes; these are alterations in which there may be an increased risk for certain cancers and cardiac conditions. At The London Genetics Centre we are only looking for alterations in actionable genes ,i.e. we will not include analysis of genes related to Alzheimer’s/dementia, as presently medicine cannot definitely change the outlook enough to balance the dark cloud of such knowledge. It will at present not include analysis of dietary genes, as current interpretation of this area is still not clear. The experts presently do not feel there is sufficient consensus to fulfil our actionable criteria. However, we think this is a really important area for the future, and we plan to increase the actionable gene list as research progresses.
Pharmacogenomics: Can your genes help choose the right medicine for you?
Medicines are absorbed through your gut, then some may need to go from an inactive to an active form; the ability to do so may be determined by your genes. Separately many medicines are metabolised and denatured in the liver through pathways which are also genetically controlled. The study of genes that control these two areas is called pharmacogenetics.
We will be sequencing your pharmacological genes to see how you specifically activate and metabolise each medicine. This may mean you will need to change the dose of a particular drug, or avoid it completely, to minimise potential side effects.
All patients will gain from knowing about their genetic pharmacology.
Chromosomes in cellular division.
(Click to enlarge)
(Click to enlarge)
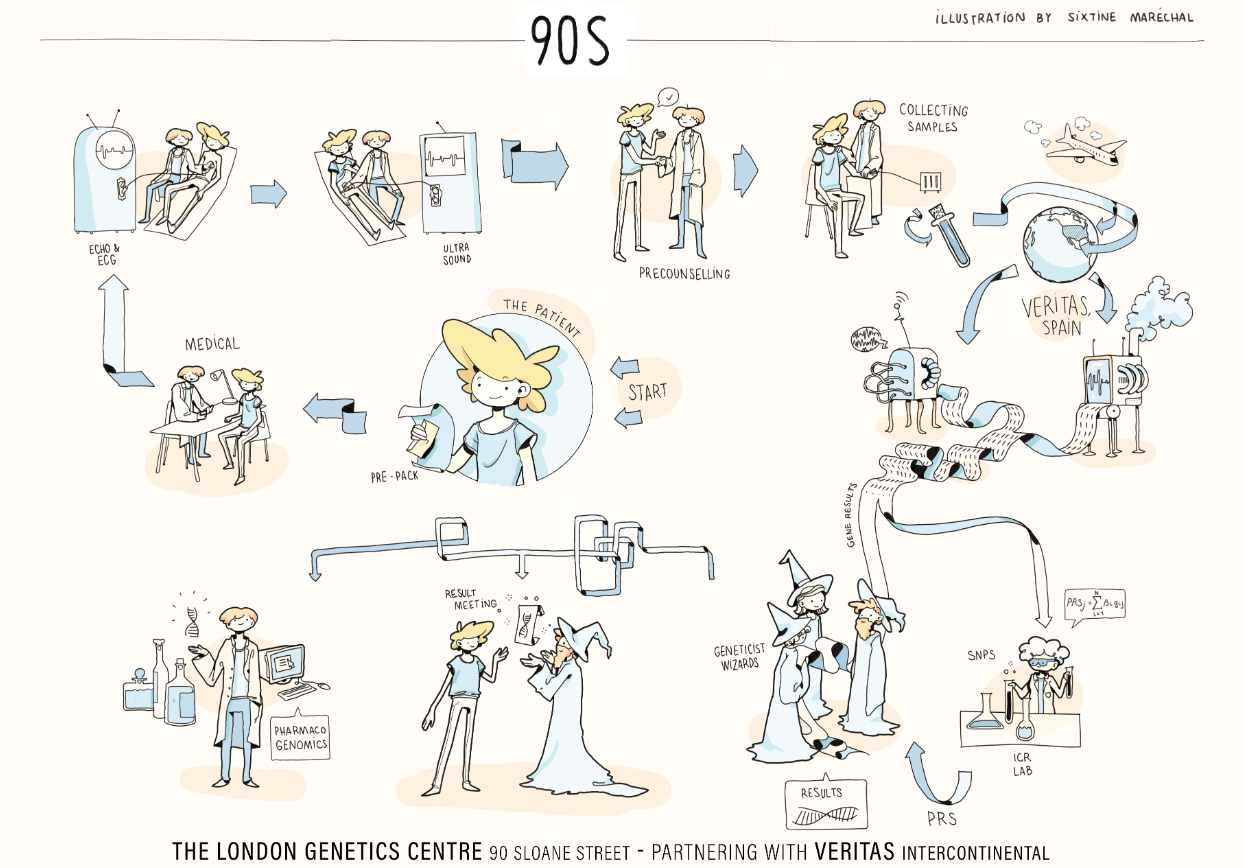
Whole Genome Screening Pathway
The Practicalities - How is it done?
The journey begins with a full Medical at 90 Sloane Street or an accepted GP partner centre. This includes a full history of current and past illnesses, together with family history and any medication taken. You will undergo a detailed examination, a blood screen, ECG, echocardiogram as well as an abdominal and pelvic ultrasound. All these tests are non-invasive and have no radiation.
We will discuss Colonoscopy screening benefits and sometimes CT coronary angiogram screening options individually but they are not part of our Whole Genome Screening.
When you apply for Whole Genome Screening at The London Genetics Centre you will be emailed an information pack.
This includes a more detailed explanation of the pathway, our Welcome Letter, a family history questionnaire to fill in and consent forms to read and for your own record. You can then email the family history questionnaire back to us and book your appointment/medical. You will have a 30-minute pre-test counselling session immediately after your medical where any remaining questions and queries about the test can be addressed and the consent forms signed. Your sample will be sent off after this. This is a 30-minute appointment immediately after your full medical, and following which your whole genome sequencing test can be sent off.
Where and Who will be conducting various aspects of the different tests?
All tests will be done at The London Genetics Centre. Other partnership practices can do the Medical part for their own patients.
You will have your Medical with a GP. The heart tests, ECG and Echocardiogram will be done by our cardiac technician. The ultrasound is done by a specialist radiologist. You receive your genome result with a Consultant Geneticist at The London Genetics Centre, this can be face-to-face or using Zoom if you prefer.
We are doing Whole Genome Sequencing as a part of best medical care with a full medical assessment.
We have developed the 'Next Generation Screening'.
Cancer genes – examples:
Breast cancer: We screen for 15 different breast cancer gene alterations, which put patients at 2-8 times the normal population risk. If you have an alteration in such genes, the age of starting breast screening and its frequency would be adjusted. This will enable earlier diagnosis and potentially reduce the risk of dying from breast cancer.
For those at the very highest risk of genetically-defined breast cancer, women can consider lifesaving skin sparing mastectomy with aesthetic combined reconstruction surgery, or more intensive screening.
Alterations in the BRCA1 and BRCA2 genes increase the risk of breast cancer, but they also increase the risk of ovarian cancer. With this knowledge, women can choose to have their ovaries and fallopian tubes removed, after childbearing years, as a life saving measure.
Men who inherit alterations in BRCA1 or BRCA2 may also be at risk of male breast cancer or prostate cancer, and will be provided with advice for risk management.
Ovarian cancer: we test for alterations in 9 genes including BRCA1 and BRCA2.
Colon cancer: If an alteration in a colon cancer risk gene is found to be present, lifesaving regular colonoscopy screening can be started as early as 25-30 years of age, depending on the specific alteration. Almost all colon cancers start with a pre-cancerous phase of colonic polyps which gradually increase in size before becoming cancerous. These polyps can be detected at colonoscopy and simply removed at the same time. Regular colonoscopies every 1-5 years can result in 70 per cent of colon cancers being prevented.
Prostate cancer genes: – Prostate cancer screening has up to now been controversial in the general population. Prof Eeles has recently published data to show that men who carry alterations in the cancer predisposition gene, BRCA2, should be offered regular prostate screening using the PSA blood test. She is also running a pioneering study Barcode1 looking at the use of SNPs for stratifying prostate cancer risk
Cardiac Genes
We are screening for a large number of actionable Cardiac genes combined with an onsite Echocardiogram – a sophisticated non-invasive way of filming the heart in action. This is a key reason why The London Genetics Centre is the place to do Whole Genome Screening.
Examples:
Cardiomyopathies- are heart muscle disorders that are not due to coronary artery disease. Genes control heart muscle development; gene alterations can cause two of the most common types of heart muscle disorder:
1) Dilated cardiomyopathy – the heart being a floppy enlarged bag.
2) Hypertrophic cardiomyopathy - the heart muscle becomes excessively thick. Some people carry certain cardiomyopathy gene alterations without developing signs or symptoms of cardiomyopathy. We carry out an Echocardiogram in all patients before the gene test which means we can tell such a patient that while they have a genetic alteration that can cause cardiomyopathy their heart Echo is normal and they do not have any evidence of the condition. We would however, occasionally repeat the Echo to check there is not any change over the years.
However, if their echocardiogram shows early signs of cardiomyopathy, knowing they have such a gene alteration means a patient can start lifesaving drugs, or treatments earlier, making an enormous difference.
Long QT genes – Inherited alterations in these genes can cause life threatening heart rhythm disorders; having the knowledge of such gene alterations being present can be lifesaving. Lifestyle advice includes avoiding certain medicines known to prolong the QT interval.
Aortopathy genes – Alterations in these genes can result in an enlarging and weakening of the aorta – the main artery that comes off the heart. Ultrasound screening for these aneurysms can identify if/when radiological or surgical procedures are needed.
Familial Hypercholesterolaemia – alterations in these genes result in dramatically high cholesterol levels. This can be treated with diet and medications, which will significantly lower the risk of heart attacks and strokes.
Actionable “non-oncological/non-cardiological genes”: a few examples:
Factor V Leiden - Deep vein thrombosis is increased 8 times by the presence of this genetic alteration, which can cause fatal pulmonary embolism (clots in the lungs). Prevention involves using anticoagulants when at risk, such as flying or post-surgery. Also we advise against the combined contraceptive pill, as the risk of clots is increased many times if this alteration is present.
Haemochromatosis - a genetic alteration causes increased absorption of iron which can result in fatal liver, pancreatic and cardiac damage. This can be easily treated by intermittently removing some blood, to stop the iron build up and its toxic effect.
Whole Genome Sequencing is the sequencing of all the DNA building blocks (nucleotides) of an individual’s genetic code. Sanger sequencing was originally used but is time consuming and expensive and it would take years to sequence all of a person’s DNA- known as their Genome. Next-Generation sequencing has accelerated the process, taking only days to weeks to sequence a whole genome.
Single Gene Analysis
This is genotyping for only a specific chosen gene: originally mainly done before Panel tests were developed. It is still used for testing family members of someone (the proband), who has been found to have a gene variant.
Panel Testing
Panel testing refers to the testing of groups of genes usually associated with particular medical conditions. At The London Genetics Centre we are doing two large panel tests, cancer and cardiac.
Cancer panels looks for germline cancer predispositions that are known to be associated with a particular cancer. They have the special gain of not missing large deletions, which can very rarely happen with WGS, but they do not have the massive wide gene coverage of WGS.
The landscape of genetic testing has shifted from single gene testing to that of multi-gene panel opened up by the continued decline in cost. In many cancer cases gene panels testing for germline genetic alterations that can cause that specific cancer are ordered. For instance, panel of genes for breast, ovarian or colorectal cancers.
The latest Breast Panels now include: BRCA 1/2, PALB2, ATM, CHEK2, PTEN, STK11, TP53 and BARD1.
In the UK, the National Institute of Health and Care excellence, sets a cost effectiveness threshold of gene testing for family history situations, where there is a pre-test 10% or greater estimated likelihood of finding a significant genetic alteration.
Whole Exome Screening
Sequencing for the DNA that provides instructions for making proteins. These pieces called exons are thought to make up 1% of a person’s genome. It is an efficient method for identifying disease causing mutations. Analysing coding areas of all genes, it will include genes such as cystic fibrosis and haemochromatosis as with WGS. It will not enable you do the SNPs nor calculate polygenic risk scores which is possible with WGS. It could also miss some carrier genes, if they are in the intronic regions.
Whole Genome Sequencing
DNA Sequencing for all the nucleotides and their order.
This will also detect DNA variations outside the Exons which are now known to affect gene activity and protein production leading to genetic disorders.
SNP profiling can be done for different conditions such as Prostate, Breast, Ovarian and Colorectal cancers and others. Cardiovascular SNP risk profiling is also being carried out to detect those at higher risk of cardiovascular disease, some of whom are not identifiable by the usual cardiovascular risk factors. At present this is in the research arena but we hope that in the near future this will be important for personal healthcare risk identification with consequent preventative actions.
Variant Classification
The American College of Medical Genetics and Genomics (ACMG) grades variants into 5 categories. Class 5 Pathogenic – disease causing, Class 4 -likely pathogenic >90% certainty of the variant being disease causing. Class 3 is a variant of uncertain significance (VUS). Typically most VUSs have about a one in a hundred chance of ever being upgraded with time to pathogenic; so some organisations do not report them as in the vast majority they cause unnecessary costs and potentially worry.
Whole Genome Sequencing leading to Polygenic Risk Scores.
Whole genome sequencing enables the SNPs to be read and their associated risks can be amassed into a so-called polygenic risk score. There are different scores for difference conditions. For example, a person with a polygenic risk score for prostate cancer on the 98 centile will have 6 times the risk of prostate cancer compared with the average of the population. Such individuals can be offered research studies investigating the role of targeted screening in such groups.
In summary, considering prostate cancer the genetic screening system at The London Genetics Centre will look for 8 major genes for prostate cancer of which BRCA genes are one part. We will also do Prostate SNP profiling to give a prostate polygenic risk score, picking up further high-risk men, extending beyond those identified by the major genes.
Pharmacogenes
With Whole Genome Screening we are also able to do the Pharmacogenes showing how we individually metabolise drugs. This is a new and developing area of medicine. Medicines and their dosing can be personally tailored for you. Also, drugs that could be potentially fatal for you, or on the other hand not effective can be avoided
Age for testing
25 years is our minimum age at present and we have no maximum. Younger patients if they have a strong family history can see a geneticist at The London Genetics Centre.
Are there people who might not be suitable for genetic testing?
Severe depression, bipolar disorder, psychosis, dementia and cognitive impairment or a lack of maturity are all relative contraindications. A history of depression, where recovery has been good, would, in the majority of cases, not be a contraindication.
Psychological effects on patients with new genetic information
We take this area seriously and will be assessing how some patients react to finding out they have an actionable gene alteration. The current evidence is that for patients who are found to have a harmful gene alteration, six weeks after being given the information, they are not more stressed than those who have not been found to have a genetic alteration. We have excellent psychological support at 90 Sloane Street, if required.
Counselling
Patients found to have a genetic alteration increasing their risk of disease will gain from our counselling, so as to benefit from the new knowledge and the preventative possibilities. Our team includes experts in genetic counselling. Unfortunately, many centres offering genetic testing simply send off the tests without a detailed network of high-level geneticists available to patients when abnormalities are found. There are only about 250 consultant geneticists in the country. The London Genetics Centre has deliberately built up a team of broad genetic expertise.
Genetic testing and Insurance
At present UK insurance companies have issued an ongoing genetics moratorium for those taking out insurance in the UK, which means you do not have to declare gene alterations that may put you at greater risk, but this excludes Huntington Disease, a degenerative neurological condition. So you do not have to declare genetic information in most circumstances. It should be noted that there are some parts of the world where there is not a genetic moratorium and patients need to declare genetic test results. We always strongly advise consulting the Code of Genetic Testing and Insurance in combination with legal advice for greater clarity on how this applies to you.
Please refer to the following key document for further information: www.abi.org.uk
If I am unable to give a blood sample are there other options?
Saliva can be a viable alternative.
The cost of the full medical and bloods, electrocardiogram and echo together with abdominal and pelvic ultrasound, pre-counselling, Whole Genome Sequencing and separate additional genetic panel tests and a 30-minute post result consultation with a consultant geneticist is £4,995. The multidisciplinary meeting of 4 geneticists reviewing your results and producing a 3 page Summary MDT sheet is currently done for free.
If you have an actionable gene alteration you will have the option to pay extra for an extended 60-minute post-test consultation with the geneticist.
How long do the results take?
12-16 weeks from the time of sending off your blood; you will receive an email to let you know your results are available. All results are given in a face to face or a Zoom consultation.
Is our whole genome screening safe and accurate?
We have spent 2 years in development, planning the logistics of every step of the process, harnessing the wisdom and experience of our world expert genetics colleagues.
Many commercial tests are designed for research/interest purposes only, and cannot be used for clinical care, as they are not undertaken with the same depth and quality control. Our whole genome sequencing test is carried out in carefully selected diagnostic laboratories. We also use blood tests as they reduce the occasional failure of using saliva.
All results are seen by our consultant geneticists. Abnormal results are discussed at a multi-disciplinary meeting of several consultant geneticists, to access the greatest knowledge and best advice.
Will I be advised on my treatment options? Will I be obliged to follow that treatment and will treatment be included in the cost?
Your response to the advice given is entirely yours, and your information is confidential.
Further screening and any treatments are not included in the cost.
Should you discuss results with your family if you have an actionable gene result?
Where you can do something to lower risk for yourself, in general terms it is usually advisable to share this knowledge with family members at an appropriate age. They can potentially benefit from the findings and our genetic counsellors will help with this process.
Confidentiality is at the heart of how we have structured The London Genetics Centre.
Data security will be our top priority.
Where will my results and data be stored?
Your data will be stored at the gene sequencing laboratory with your consent.
Can I have my results anonymised or destroyed after the test?
Yes, all samples and results can be anonymised. You can ask for your sample to be destroyed at any time – it is your sample.
Will my results be used in any generalised research?
Your test sample and the forms that we send off as well as the results are anonymised. This is for patient confidentiality and protection. Anonymised research is carried out by the sequencing companies and this is why we anonymise at the start of the process at The London Genetics Centre. Also, anonymised research may be done by The Royal Brompton with your consent. Your anonymised data, if necessary adjusted to stop any chance of identification may be used for audit purposes or in summary result documents. With permission, we do show some unidentifiable results on our web site or brochures to help as this is a new research area.
Will I be able to access my data and move it elsewhere for further analysis?
Yes, the results are yours.
Is this the ultimate test or will there be more to come?
Further disease-causing genes alterations will be found and we will learn more about the effects of combinations of genes and SNPs. Sequencing reads may go to a greater depth and this may reduce the miss rate from one in several thousand, at present, to even lower.
We are already reducing any miss rate by going to greater depth in targeted areas.
Your current genome reading itself will not change, but there will be more knowledge about genes, particularly in the setting of the healthy population.
Also, our understanding of VUSs (variants of unknown significance) will increase. This means it may be worth reviewing your genome in years to come to harness new genetic knowledge, as it applies to you.
How will pharmacogenomics impact healthcare in the future?
In time, genetic pharmacology will be a vital tool for doctors. Your medical computer record will include the details of your genetically governed pathways. Your doctor’s computer will automatically give prescribing advice to your doctor when a medicine is prescribed. This will make medicine prescribing safer and doses correct for you.
Please email enquiries@TLGC.uk and we will email you back.